Joraaver Chahal
What I'm Learning about Osteoarthritis: Part 1
May 14, 2024Reading Time: 6 minutes
Last time I posted, I was anticipating being able to dunk before my 30th birthday. That train was derailed by a bout of swelling I had about four weeks ago. Since my ACL surgery in 2020, I’ve had about three bouts of knee swelling. The most deleterious bout of swelling occurred while playing volleyball at an open gym. After landing from a block, I heard a large crunch in my knee and it became a tad unstable, but nothing I couldn’t play on. I knew it wasn’t my ACL. The next few days required swelling management 101, and it took about two weeks for it to settle before I could assume normal training and playing. It took four weeks before I could see my sports doctor, but by then I had about 95% function, with the only problem being the occasional catching in my knee. We settled on a possible mensicus tear, but no MRI was ordered due to my current level of ability.
It never put a serious dent in my athletic pursuits, but the latest episode of swelling four weeks ago gave me cause for concern. Not in the swelling’s mechanism, but in it’s timing and the reality that it presents. My ACL surgery included a partial lateral menisectomy (small removal of the lateral meniscus), and if I have another active tear, then my risk of Osteoarthritis continues to increase. I’ve always known that I’m higher risk of experiencing Osteoarthritis due to my ACL surgery, menisectomy, and higher bodyweight. However, my continued participation in an intense jumping sport spurred my decision to educate myself on the subject.
I’m no Luis Suarez but if I’m too reckless with my pursuits I’ll end up in a similar place.
That said, I picked up the ESCEO Atlas of Osteoarthritis to gain a broad understanding of the topic that affects millions of people. Much like with my Patellar Tendinopathy, I have a tendency to go deep on a singular topic, so what I write tends to be translatation of notes I’ve made for myself on the subject.
Unlike my previous post on Patellar Tendinopathy, I will break this post up into multiple parts, so I don’t write a tedious thirty-minute essay. This first part is dedicated to just understanding what Osteoarthritis is and how it is diagnosed, from a clinical perspective. I don’t intend to dwell on the subject because I’m no expert, and like I said above, what imaging reveals is not necessarily an indication of function. Nonetheless it’s a tool to learn from and understand, as long as it is not abused.
History of Osteoarthitis
I’ll keep this short, sticking to only the interesting.
The first recorded study of cartilage was by a Greek philosoper and physician named Galen in the year 175. It’s amazes me how long ago initial study of the subject occurred. We stand on the shoulders of giants.
Initially Osteoarthritis was treated as a cartilage only disease. Now, due an increased understanding in how many systems and tissues are affected by the disease, Osteoarthritis is considered a whole-organ disease. There are changes affecting multiple tissues as the disease progresses, and it is impossible to treat one in isolation without considering the rest. To put it in one sentence:
Osteoarthritis is a whole-organ disease in which there is a general degradation of a joint’s ability to function due to abnormal changes in the multiple tissues that make up the joint.
This definition falls a little short in the “due to” phrase because of the inability to 100% correlate image findings with function, but it is a starting point that most can rely on as a strong mental model for the condition. Note that there is no mention of it as a “degenerative” disease. To quote the reference material directly:
Osteoarthritis is often thought of as a degenerative condition, but does not arise just because of gradual wear and tear. Instead, it should be looked at as an abnormal remodelling of the joint tissues, articular cartilage and bone, which is driven by many inflammatory mediators. -Atlas On Osteoarthritis, 2nd Edition
Diagnosing Osteoarthritis
Symptoms
These are easily identifiable and track across most people experiencing Osteoarthritis in a particular joint:
- Warmth
- Swelling
- Stiffness that goes away with activity
- Pain
- Instability
- Deformity
- Altered usage patterns
These are usually indicators of joint problems, regardless of the condition, but the symptoms above become consistent and increasing depending on the severity of the condition. For example, pain is an interesting symptom. At first there may only be stiffness. But gradually, pain upon movement occurs until the joint is “warmed up.” And when the condition is severe, there may exist pain when the joint is at rest. Stiffness may occur in the morning only, but also become more present throughout bouts of stillness. Deformity and altered usage patterns are usually noticeable only much further down the road.
Imaging
The gold standard in imaging is a simple x-ray, or radiograph. However, the variables that tick the boxes for an official diagnosis of Osteoarthritis aren’t well agreed upon, especially in earlier stages. These are the current tools used when examining a radiograph of a possibly osteoarthritic joint:
- Joint space narrowing (JSN)
- Osteophytes
- Subchondral sclerosis
- Cysts
A grade called the Kellgren-Lawrence grade (a.k.a KL grade) uses a combination of the above factors to produce a score from 0-4 to determine the severity of the condition. It is referred to in many papers as well when studying the disease’s progression and possible interventions.
To maximize understanding of the grades, here’s an image from a research paper about using machine learning to automatically classify imaging of a possibly osteoarthritic knee joint:
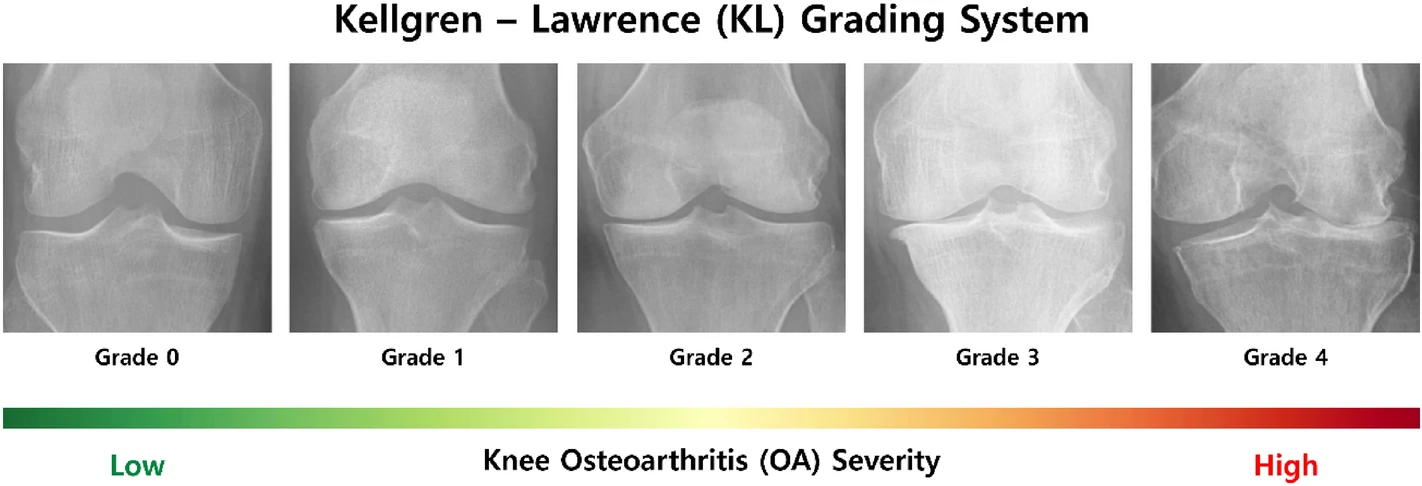
Looking for all the variables listed above may be difficult to the untrained eye. The easiest ones to identify when comparing a grade 4 vs grade 0 joint are joint space narrowing and the presence of osteophytes. I’m not going to go into the details of how to identify the variables and what the thresholds are (because I am not trained in the reading of said images either) but note that the criteria exist.
The biggest takeaway to address from this portion of the atlas is that when individuals come in with pain due to Osteoarthritis, the joint may already be grade 2 or 3. Pain comes well after deterioration of structure, but sometimes there is no pain. That’s what makes tackling the disease so difficult to begin with. The imaging alone isn’t enough to justify an intervention, so it’s justification as a prognostic tool is weak.
In the next part I’ll discuss the clinical factors involved in how Osteoarthritis progresses, before diving into treatmenting the condition.
#training #injury