Joraaver Chahal
How I Recovered from Debilitating Jumper's Knee
Oct 22, 2023Reading Time: 23 minutes
TL;DR:
- If it’s acute, recovery is easy. Just rest and it will recover. Then ramp up your volume. You will succeed.
- If it’s chronic, recovery is a long process. Stop playing sport and start your rehab. But you have to be all in. A wishy-washy rehab will take you nowhere.
- If you can’t stop playing your sport, then work with your coach to make sensible changes. Track jump volume. Do isometrics or slow lifts before/separate days of practice.
- It’s emotionally draining at the start, but when you start to see changes, everything will click. Give it 6-8 weeks to really see the impact of proper rehab.
Why Write About This?
I wanted to write about this because I have a very good technical grasp of the problem as well as the emotional and physical toll Jumper’s Knee has on an individual. I’ve recovered from it and coached others to return to sport from it too. My journey includes its own peculiarities that some may find useful.
Another reason is because I wrote this post two years ago. Do I feel silly for suffering from Plantar Fasciitis (a story for another day as well) and Jumper’s Knee after writing it? Absolutely not. Nobody said writing about my injuries or “expressing humility” was going to make me more resilient. I still play my heart out when I step on the field. I just calibrate to injuries faster, become less emotional about them, and am now a far more valuable resource to others because of them. That is why I write.
How this post is structured
- What is Jumper’s Knee (and does it affect you?).
- How I got Jumper’s Knee
- How I rehabbed Jumper’s Knee.
- Where I am now.
This article will be long and in-depth. I will address the above points in a factual fashion first, and then add my perspective as a patient. I do not touch on the science behind why certain aspects of recovery work. It burdens you with additional knowledge that has no bearing on your ability to recover. If the reader wishes to know more for his or her personal gain, just contact me and I can forward the sources. Podcasts, research articles, etc. You can save yourself some time and look up “Jake Tuura.” He has all the answers.
I will also avoid as much clinical terminology as possible. I will only introduce it if, in your attempts to find out more about the problem, these terms come up and it behooves you to know them rather than run from them.
With that, let’s begin.
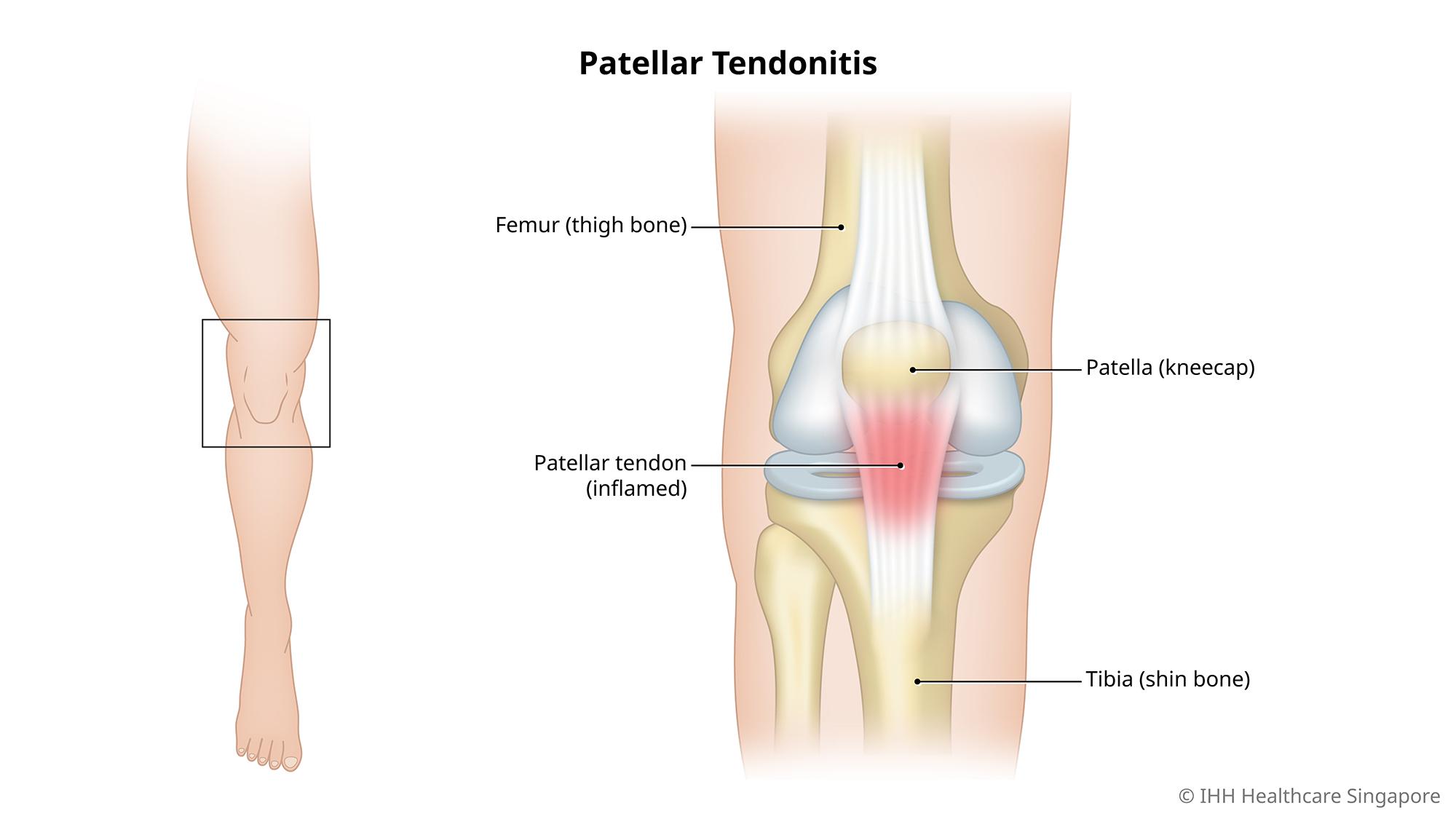
What is Jumper’s Knee
First, its clinical term is Patellar Tendinopathy. The patellar tendon starts at the kneecap and ends at the top of the shin bone.
Second, its symptoms are simple:
- Your pain is either at the top of the patellar tendon, just below the kneecap, or your pain is about 2-3 cm below at, at the end of the tendon.
- If it is at the top of the tendon below the knee cap, you can press and make it hurt with ease.
- Your pain begins as a slight soreness in the morning that goes away with a little warm-up, but over the course of a few months it becomes a constant pain, occurring during sport or walking down the stairs.
- You participate in an extremely heavy jumping or cutting sport.
Third, it’s cause is best summarized by Jake Tuura as follows: “it’s always a load issue, and sometimes it’s a biomechanics issue.” What he means by that is an individual suffering from Jumper’s Knee might have tight or weak muscles leading to improper movement patterns, or have none of that. Regardless, the sufferer went from doing little or no jumping or cutting, to doing a lot of jumping or cutting, in a very short amount of time. That spike in volume brought on the condition.
If these apply to you, you have Patellar Tendinopathy, a.k.a. Jumper’s Knee.
The condition is “acute” when the symptoms have been present for less than 2-3 months. Any more than that and the condition is considered “chronic.”
If you, like me, did more research, you will find that some classify the tendon’s state in more detail. One such category is “degenerative.” Throw this vocabulary out of your head. It only matters to a clinician and has no place in a patient’s mindset. Don’t add unnecessary emotional drama; it doesn’t change the process.
How I Got Jumper’s Knee
In 2019 I tore my anterior cruciate ligament (ACL) in my right knee. A day before my birthday, in fact! In January of 2020 I had ACL reconstruction done using my patellar tendon on my right knee. I was aware that I was at a higher risk of getting Jumper’s Knee given that a piece of my tendon was missing. However, I had very little guidance during my rehab, so just note that it wasn’t easy to tell if the front knee pain I felt was from the surgery or not. I passed my return-to-sport testing for ACL reconstruction even though I told the physical therapist I was in a considerable amount of pain. There is a lot to unpack about this particular point, but it’s an article for another day.
I started playing more volleyball in the summer of 2021 and continued to experience a little bit of pain. At this point, while I was well past return-to-sport guidelines for ACL reconstruction (9-12 months), front knee pain due to a patellar tendon autograft can last a long time. Unfortunately, as I played more, it became apparent that the pain was increasing. That and I realized all the above symptoms checked out. A whole year had passed since the start of this ongoing battle. So in the spring of 2022 I did the hard thing. I admitted to myself that I had a serious case of Jumper’s Knee and stopped playing all volleyball.
How I Rehabbed My Jumper’s Knee
I started with a visit to physical therapy. 15 Step Downs later and I felt no better, nor was I given a recipe for success. Let this be a lesson to you all. Classic, insurance-based physical therapy and tendinopathy do not mix. You will learn why towards the end of this article.
After an underwhelming physical therapy experience, I took it upon myself to understand everything about my problem. To be brief, everything I know can be attributed to Jake Tuura’s videos on fixing patellar tendon pain. He is one of the best at distilling information from the world’s most knowledgeable researchers, like Jill Cook and Keith Baar, and informing the common athlete. Here’s what you should know:
- Tendon changes can take a while to feel different due to their lower blood supply.
- Heavy slow resistance work has been shown to improve tendon quality AND improve patient adherence.
- Next day pain matters the most, but depending on where you are in terms of pain, adjust expectations.
- When the knee starts to feel good during day to day activities, jumping MUST be reintroduced over a 4-8 week period depending on needs.
- Once bitten, twice shy. If you’ve had the condition, the condition is more likely to return. Stay vigilant.
Now comes my personal experience.
First of all, stopping all sport is rough. Especially if it’s your main social circle. If you are an athlete and this is your first major injury, it’ll challenge your identity. If you feel empty without your sport, begin to isolate yourself from your teammates, or get angry because you feel like those who ask after your health are pitying you, then it’s as I said. I’ve experienced this. But Jumper’s Knee isn’t career ending, so take heart. Regardless, you may want to read this.
I’m fortunate enough to have a twin who experienced the same issue, so I wasn’t alone in the process. However, watching him play volleyball for our team while I watched from the sidelines was hard. But after having torn my ACL, I was familiar with the concept of stopping sport and how that would affect me. Like I said in the beginning, it’s not a question of whether or not you’ll be injured, but how you respond to the fact that you are injured. So I buckled up and decided I was in it for the long haul.
After consuming all of Jake Tuura’s three minute lectures on different aspects of fixing Jumper’s Knee, I bought his book “Jumper’s Knee Protocol” or, has he refers to it, JKP. I combed through that and started to experiment with my rehab plan. I use the word “experiment” with great intention.
Stage 0: Movement Assessment
Biomechanics may be an issue. There are valid reasons for believing that limited ankle mobility, tight quadriceps musculature, or limited hip mobility could attribute to additional load on the patellar tendon.
I knew I had three long standing issues, in order of importance:
- Reduced right calf strength post ACL reconstruction.
- Reduced left ankle mobility.
- Slightly reduced right hip mobility.
The calf strength was evident to me during my return-to-sport testing after my ACL rehab, but not to my therapists. Based on my injury history, I concluded that my tendon was highly aggravated due to strength deficits in the quadriceps and calf complex and an overload of maximal jumping. My left ankle mobility restriction likely increased the load on my right knee, but I marked it as a secondary problem, to tackle later.
I gave my sport some thought too. Most of my jumps occur in two forms: double leg jumping and landing, such as during most block jumps, or double leg jumping and single left-leg landing, such as during more powerful hits. As middle blocker, the landings are stiff, meaning decreased time to disperse energy. And no, you can’t tell a middle blocker to “land softly.”
Telling an athlete they are “landing incorrectly” during sport is meaningless. Outside of sport, in non-chaotic environments, training an athlete to only land a certain way ingrains useless patterns. Exposure to only “correct” movements suggests that the instant an athlete enters a position different from that, he or she is doing something “wrong” and is bound to be injured. Hindsight bias wins. That’s a fragile mindset. Get rid of it. Instead, adopt the mindset that an athlete is strong in what he or she is exposed to frequently. Expose athletes to different landings, chaotic landings, unplanned landings. In this way, assessing an athlete’s movement becomes less of a snapshot in a single point in time, and more of movie reel accounting for all their previous movement experience.
Stage 1: Isometrics
The first recommendation when everything causes pain is isometrics. An isometric exercise involves holding a muscle at a fixed length and contracting it for a certain period of time. Because they involve no movement, isometrics make it easy to find a position that does not provoke the tendon while strengthening the rest of the tissues involved.
I must reiterate, isometric exercises are used when the tendon is considered “fragile” or is easily provoked. As I just said in my case, everything hurt. If this does not sound like you, isometric exercises do not need to be your starting point. You might find the Stage 2 exercises more suitable for your needs. The best exercise recommendations for isometrics are Spanish Squats and Machine Leg Extensions.
Let me be clear. I could not walk down stairs without pain. I could not sit for thirty minutes without pain. I couldn’t push my foot against anything without pain. Before it got this bad, I could do lunges with 120-140 pounds. However, this was due to the warmup effect, where I would start hitting heavy weights too quickly because I “felt good” in the moment.
This is when my peculiarities began to surface. For whatever reason, my surgical knee could not tolerate Leg Extensions at all. It had nothing to do with my tendon. I felt pain in weird places in my knee that encouraged me to not risk trying it again. It worked quite well for my twin during his rehab, so I was disappointed. Luckily, Spanish Squats did help with pain relief with no negative consequences. When I mentioned that I used the word “experiment” with intention, I refer to moments like this. One exercise did not work for me. Another did. Your mileage may vary, just keep experimenting.
I did 5 sets of 45 second holds of the Spanish Squat with 60-120 seconds of rest, starting with just bodyweight. That alone was enough to make me feel better for about an hour or two. I did those twice a day religiously for 4-8 weeks. So from about June to August all I did was isometrics.
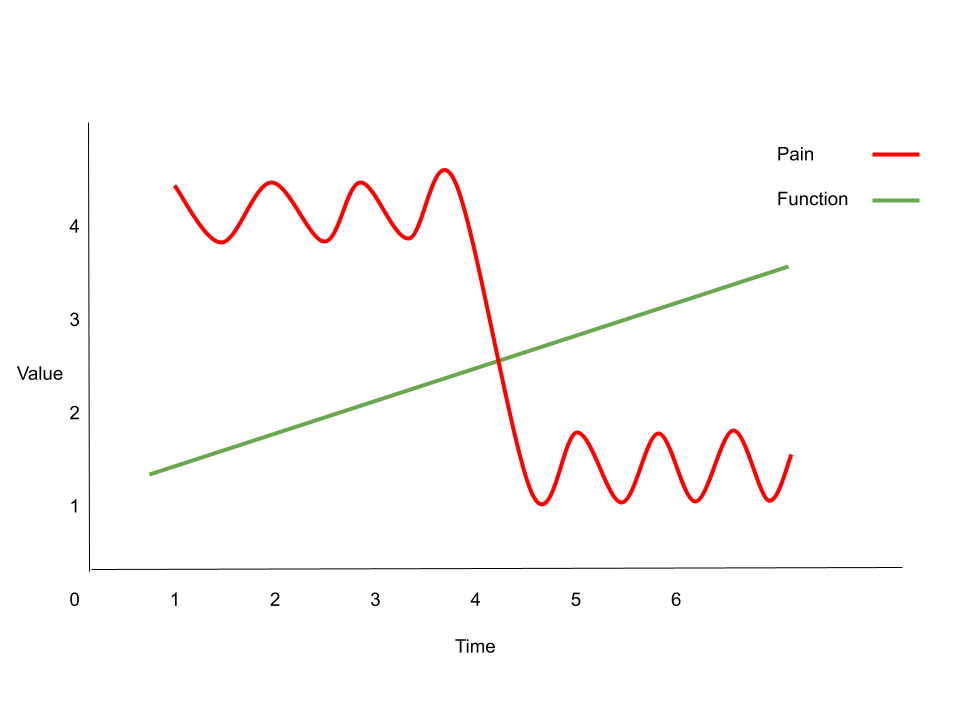
Fragile, easily provoked tendons can take 6-8 weeks of diligent rehab before changes are felt. This tracks with my experience. Do not give up if you feel nothing has changed. Tendon function is like a step function. You’ll feel nothing change until, overnight, you feel everything change. Take it all in stride.
Stage 2: Isotonics
Isotonics is another word for regular exercises. A squat is an isotonic exercise. When you move the muscle through a certain range of motion against resistance, that’s an isotonic.
Heavy slow resistance is the current best-supported practice for tendon healing. This means intentionally loading an exercise with heavy weight and slowing it down so there is no explosive component to it.
The exercise recommendations for heavy slow resistance are Bulgarian Split Squats (or Split Squats of any kind), Knee Extensions, or Leg Press. Some will tell you to do Step Downs for your condition. It didn’t work for me. It might work for you, but I don’t recommend it. In my opinion, it’s not just about which exercise is the “best”. It’s about which one you can adhere to. I find that working towards heavy slow resistance training was just a better experience than doing tiny Step Downs. Research backs this up too. Heavy slow resistance training allows for tiny increments in weight too, making progress much more visible, thus promoting a “feel good” response, even if the pain doesn’t feel like it’s changing.
When beginning movement based exercises, range of motion is a key parameter worth experimenting with. One exercise might not work if you let the knee drift too far over the toes, but by keeping the shin angle extremely shallow, it begins to work. Or working in just a partial range of motion, like going to only 70 degrees in your Split Squat, instead of 90, might help you make progress.
A big component of this stage is understanding that pain requires context to be a useful metric for progress. In Jumper’s Knee, pain that settles down after 24 hours after activity indicates proper dosing. If you feel more pain during or after the exercise or later in the day, that doesn’t mean the exercise wasn’t right. Most research suggests keeping pain during exercise to a 3/10 during rehab. However, my experience required doing exercises in zero pain. If I had pain during the exercise, I had more pain the next day. This could be due to how easily provoked my tendon was. Down the road my condition improved, but I stuck to the no pain guideline to avoid a relapse, even if it meant slightly less optimal loading. While your experience with pain during or right after exercise may need fiddling with, pain 24 hours later is still the golden rule of this stage of rehab.
At the end of each of Jake Tuura’s videos, Jake says, “Try it, see if it works for you.” I cannot stress how important this one sentence is; I feel too many people gloss over it. There are many variables you can play with like exercise selection, load, range of motion, and volume. Don’t lose faith because one combination of those doesn’t work.
On that note, I tried all the recommendations. None of them made me feel “good.” This was again, discouraging. After all, Jake Tuura touts the Leg Extension as the gold standard of patellar tendon rehab. So I took a look at all my options, and landed on this machine:

Machine Leg Press is its name.
I started with the lowest weight that was pain free. 20 lbs. Embarrassing. I could probably do 120 lbs in excruciating pain. But that would be my ego talking. My ego was getting in the way of rehab, so I shut it down fast. I used a very shallow shin angle and a small range of motion too. My feet were placed high up on that pad, and I barely hit 90 degrees when first doing the exercise.
Here’s what you have to know about rehab. When you start at the bottom, it doesn’t feel like a workout. You go to the gym, you come back, and you feel as if you’ve done nothing. But that’s the spectrum of rehab and training in a nutshell. Changes are happening to the body. Remodeling is taking place. But the metabolic systems are not being taxed in any way, even if the musculoskeletal system is. That’s the logical understanding. But emotionally, you aren’t going to have a great time. I didn’t. You just have to trudge through.
I looked back at my training logs, and it appears I didn’t have the wherewithal to write such pitiful numbers down. For the large majority of August I went from 20lb to about 90lbs, doing 4 sets of 8 reps, largely pain free and with increasing shin angle and range of motion.
Does that sound like impressive progress? Don’t be so surprised. Once you get the pain under control, you will see the weight move. But make no mistake, that is not strength you’ve gained. It is what happens when you stop provoking your tendon and load it in a pain-free and healthy manner.
If you are like me, you are in this position not only because you jumped a lot, but because you did so while being weak. Rehab exposes your weakness. I began to find 4 sets of 8 reps doing 3 seconds down, 3 seconds up with 100lb on one leg taxing. That had to change. Here is my training log from the end of August till January 11 2023 (read it from the bottom up):
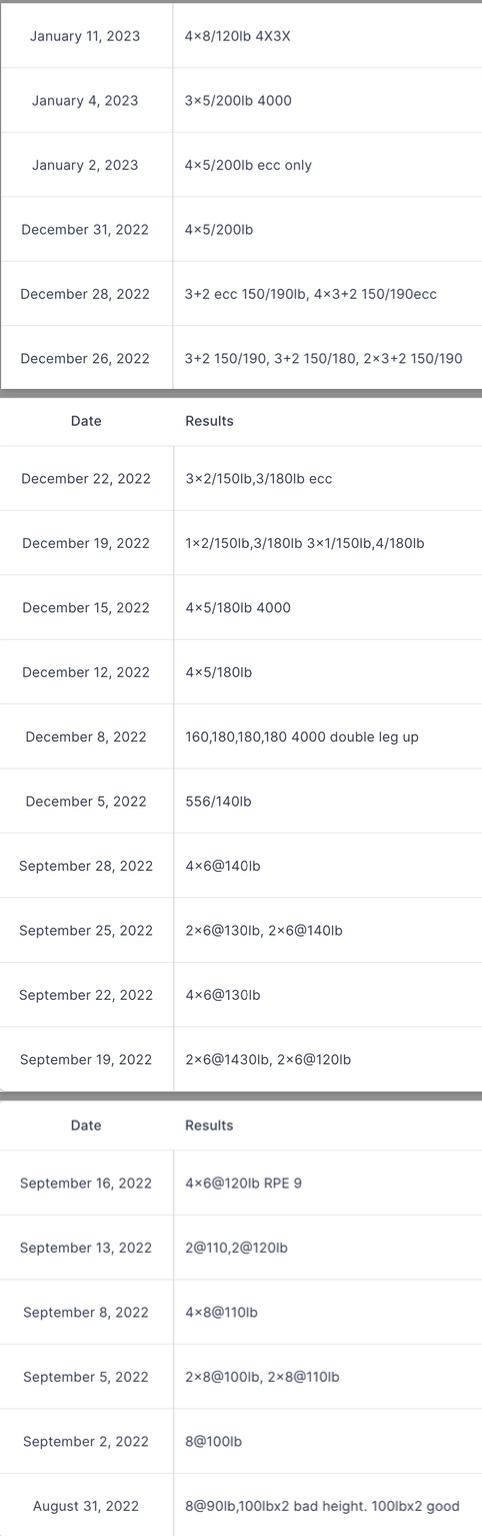
From August to early December, I was making good progress. Any lifter would be envious of such easy progress. But that’s what tendon rehab looks like if done well. The pain didn’t change during those weeks, but function was improving hand over fist. Then, in mid December, I committed to playing in the Winter 2023 Industrial Volleyball League (IVL) season. I decided that my eccentric needs far outweighed my concentric needs. I didn’t care for how high I jumped. I just needed to be able to handle 80+ landings a night. My decision to switch was also influenced by research on the specificity of training regarding eccentric only training vs eccentric concentric training, in which the concentric group got better at concentric based testing. I surprised myself with how much progress I made in those 4 weeks, handling up to 200 lbs eccentrically for 4 seconds for 3 sets of 5. January 10th, 2023 was our first match.
If you take one thing away from this stage in your rehab, it’s that you must experiment with the exercise selection and dosage to understand what works for you. Try to be as detached as possible from the inability to do an exercise. Just keep trying different exercises and differing loading parameters until you feel good. Then latch on to that and don’t let go.
Stage 3: Jumping
This is an often forgotten stage. Jake Tuura has a whole video on it.
It’s not enough to get strong. You have to start jumping again to train the tendon to handle jumping. So that’s what I did. But even here I was methodical.
In the middle of November 2022, for two days a week, I started jump training. This gave me about 6-7 weeks before my first game.
I mapped out exactly how often I would be jumping as a middle blocker by using these two sites as resources: Science Untangled’s article on Jumping in Volleyball Matches and Coaching Volleyball’s article on Looking at Jump Count
Here are the main infographics reproduced:
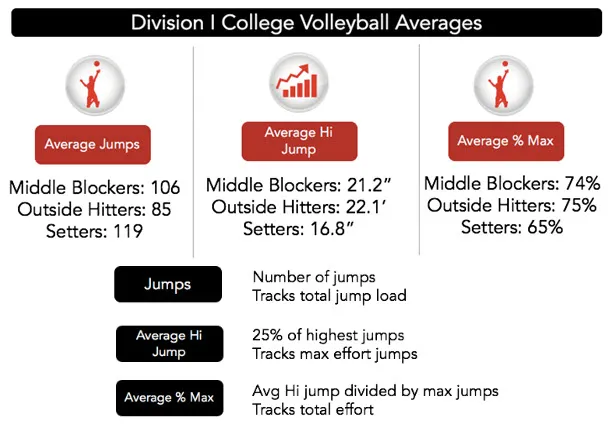
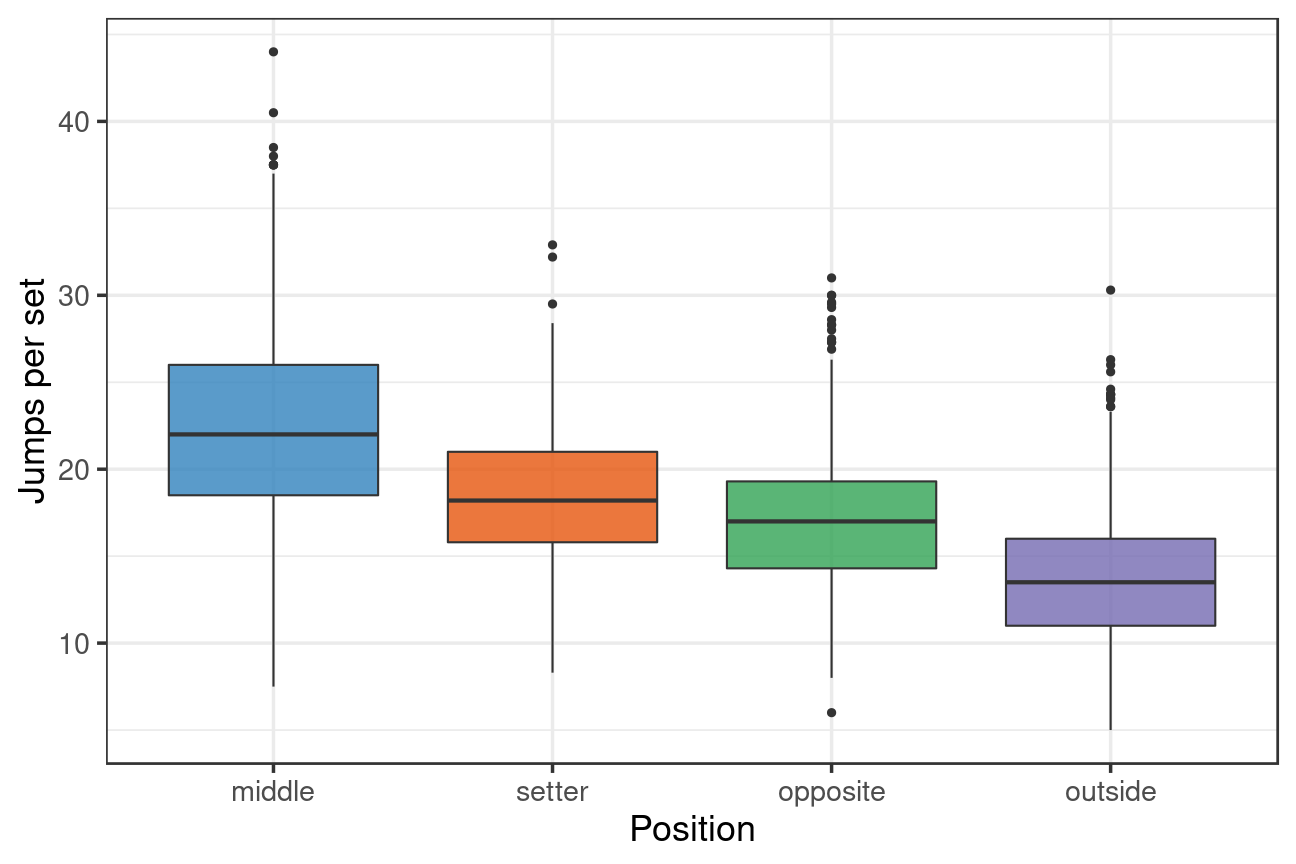
Our game nights were four sets, so I decided that reaching 80-100 maximum jumps with no pain the next day would deem me ready. I worked backwards from there. As always, I stuck to the principle of volume first, then intensity.
- Bilateral hops at 70% jump effort, 20 reps -> 50 reps
- Bilateral hops at 85% jump effort, 20 reps -> 50 reps
- Bilateral hops at 100% jump effort, 20 reps -> 70 reps
- Max effort approach jumps, 20 reps -> 50 reps
- Max effort block jumps, 20 reps -> 50 reps
- Max effort transitions (swing block jump, back off net, approach jump) -> 40 reps to 100 reps
If this starts to look less like jump training and more like conditioning, you’d be right. I was jumping to jump more, not to jump higher. So of course the goal was to handle a maximal amount of volume.
My early training also included some split landing work, but only a small amount. I mentioned earlier about the takeoff and landings involved in my sport. Very few were going to by right leg single leg landings. In the next section you’ll understand why that matters.
My training is tailored to my sport too. A soccer player would not train like this. Tailor your training to your sport to rebuild the neuromuscular skills and patterns in order to avoid injury.
Stage 4: Return to Sport
By the start of January, I had completed my training. But I was still nervous. Here were the thoughts in my head before returning to sport:
- My jump training could be completed in 30 minutes. My games lasted 2 hours. Will the rest of the ground contacts I have during the game negatively impact my knee?
- My twin returned to sport in a different manner. He was much stronger than me when he returned, and he gradually increased his time on the court as an outside hitter. I would be play full time from the get-go. I trusted my training to make me sport-ready from a general preparation perspective, but for Jumper’s Knee, I was about to find out.
- If this didn’t work, I’d have wasted my time and my money. My team would need a sub for me for the rest of the season. I didn’t want to be on the sidelines again, nor did I want to let my teammates down again. Serious rehab means not rushing things when you aren’t ready and stepping out onto the pitch with confidence when you are ready. Showing up only half-ready wouldn’t reflect well on me.
Given all the points above, I even filled out a questionnaire to put my feelings into a quantitative measure of readiness. This is known as the VISA-P.
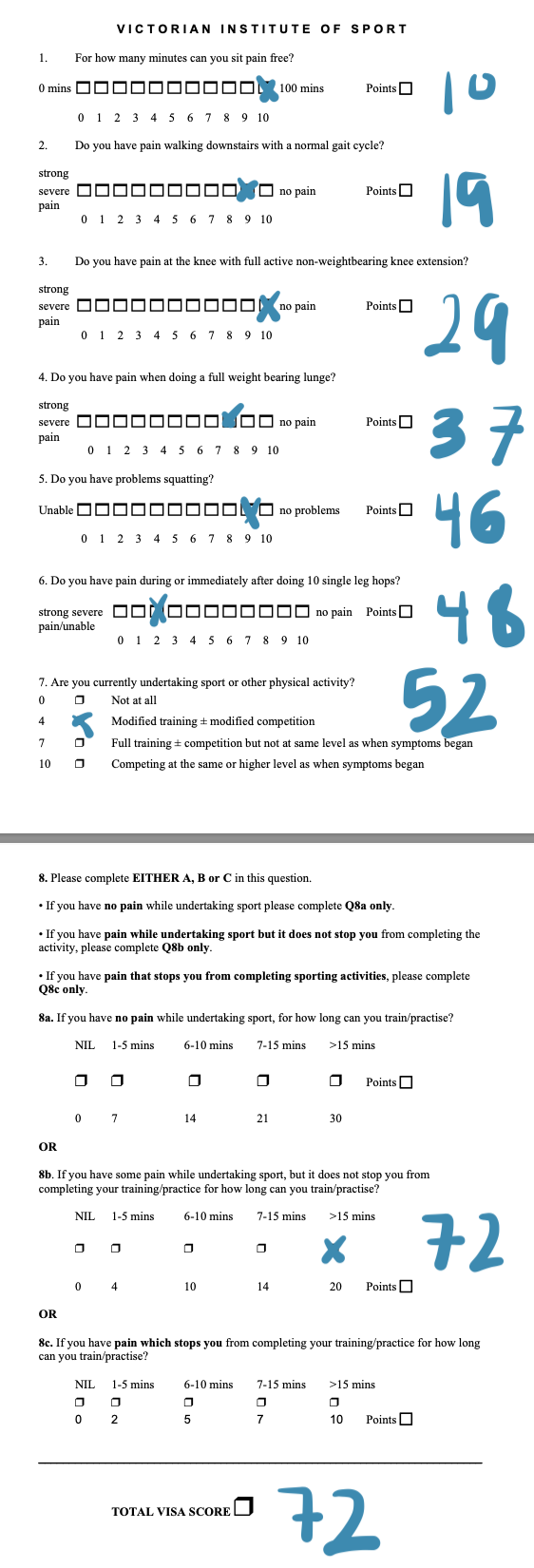
I haven’t seen many individuals discuss or use the VISA-P. However, it did expose a glaring weakness in my single-leg hopping confidence. To this date, single-leg jumping scares me the most. I’m working on it, starting with horizontal bounding, but it’s still a work in progress.
Fortunately, I was over-prepared. I woke up the first morning after our league games with no pain. After a few more weeks of playing, I decided to forgo the patellar tendon strap too. I never wore it during my training, why should I need it for my sport? If anything, it was an emotional blanket, and it felt good to let it go.
Where am I now?
I’ve been playing volleyball two to three times a week as a middle blocker or outside hitter. The only times I say no to volleyball are to stick to the rule of no back-to-back days. General guidelines suggest no more than three times a week of heavy sport and never back-to-back for returning to sport from Jumper’s Knee.
Here’s my progress on that same exercise:

It took me four months to go from nothing to 3 sets of 5 reps of 150 lb with 180 seconds rest at about a 2 second down, 2 second up pace, and then another seven months to up that to 160 lbs. That’s not great progress. However, given that I never stopped playing volleyball two-three times a week, and only proceeded to get stronger, jump higher (for another post), and get better at my sport, it’s a win-win in my book.
I took another VISA-P at the beginning of August too:
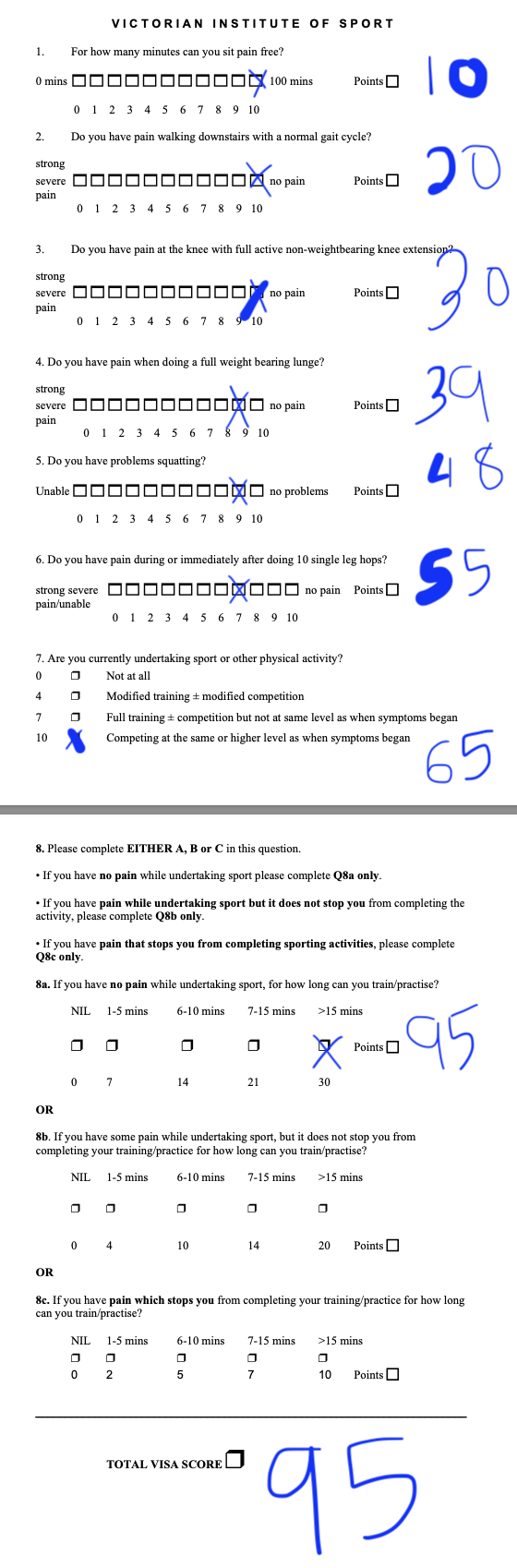
As you can see, I am now much more confident in my hopping abilities. Single leg hopping isn’t perfect, but my confidence and perception of pain are improving too.
Summary
If I could do it again, what would I change?
Stop playing sport and start rehab sooner.
That’s what Jumper’s Knee boils down to. It’s simple. I would have had less rehab to do, experienced less pain, and returned to sport slightly sooner. After all, my programming was not complicated.
The hardest part of this journey is the emotional aspect of it, not the physical.
It impacts our ability to socialize and participate in activities, which can then eat into our mental health. Many educated individuals like Jake Tuura have simple four or five step protocols that outline precisely what you have to do to return to sport. What makes personal training for conditions like Jumper’s Knee valuable is the ability to reassure the athlete that what they are doing is working, even if nothing changes. If you are going through this alone, then it requires a certain amount of faith that the process will work as well as the resolve to do the work when you see no progress. Insanity is doing the same thing over and over and expecting different results, right? Well it might feel like you are going insane, but that’s exactly what you have to do with conditions like Jumper’s Knee. Besides, you likely will see improvements in “function,” like adding a little more weight in your exercises, even when you notice no change in daily existence. But if you don’t have experience with injuries and this is a totally new domain to you, it can be a frustrating experience. If that happens to you, talking with an experienced individual can change everything.
What’s next?
I hope to dunk in the future. My approach vertical when I’m so warm I match the sun’s temperature is 10’5’’. Stay tuned.
#training #rehab